

Background: SCD is an inherited blood disorder characterized by hemolytic anemia, endothelial damage and acutely painful VOCs that cause chronic and potentially life-threatening complications. P-selectin is an adhesion protein that plays a key role in the multicellular interactions leading to a VOC. The Phase II SUSTAIN study showed that crizanlizumab (SelG1), a humanized monoclonal anti-P-selectin antibody, reduced the annualized rate of VOCs leading to a healthcare visit by 45.3% vs placebo (P=0.01) in SCD patients (pts) [Ataga K et al. N Engl J Med 2017].
Aims: To evaluate the pharmacokinetics (PK) and pharmacodynamics (PD; ex vivo P-selectin inhibition) of crizanlizumab (SEG101), as well as safety and efficacy in SCD pts with a history of VOCs.
Methods: SOLACE-adults is a Phase II, multicenter, open-label PK-PD study that enrolled SCD pts aged 16-70 years who had experienced ≥1 VOC in the 12 months prior to study start (NCT03264989). Pts received crizanlizumab by intravenous infusion over 30 minutes at 5.0 mg/kg or 7.5 mg/kg on: Week 1, Day 1 (Wk1D1); Wk3D1; and then on D1 of every 4-wk cycle. PK and PD assessments were performed in all pts pre- and post-dose on days 1, 2, 4, 8, and 15 of the first dose (Wk1D1) and then on days 1, 2, 4, 8, 15, 22 and 29 of the fifth dose (Wk15D1). Adverse events (AEs) were evaluated based on MedDRA v22.1 and AE severity based on CTCAE v5.0. Pts were continuously monitored for VOCs, with the relevant medical and treatment information collected in case of occurrence.
Results: A total of 57 pts were enrolled: 45 received crizanlizumab 5.0 mg/kg (female, n=25 [56%]; mean [SD] age, 32 [13] years) for a median of 65 (range, 6-90) wks and 12 received 7.5 mg/kg (female, n=6 [50%]; mean [SD] age, 27 [12] years) for a median of 43 (range, 9-49) wks. In the 5.0 and 7.5 mg/kg arms, respectively, 6 (13%) and 2 (17%) pts discontinued treatment, primarily because of patient decision (n=4; 9%) in the 5.0 mg/kg arm and because of death and AE (both n=1; 8%) in the 7.5 mg/kg arm.
The most common AEs were headache (5.0 mg/kg, n=11 [24%]; 7.5 mg/kg, n=3 [25%]) and pyrexia (5.0 mg/kg, n=9 [20%]; 7.5 mg/kg, n=2 [17%]). Grade ≥3 AEs occurred in 18 (40%) pts in the 5.0 mg/kg arm and in 2 pts (17%) in the 7.5 mg/kg arm. Serious AEs were reported in 11 pts (24%) in the 5.0 mg/kg arm and in 1 pt (8%) in the 7.5 mg/kg arm; none were deemed drug-related. One pt in each of the 5.0 (2%) and 7.5 mg/kg (8%) arms discontinued treatment because of AEs. Infections, infusion-related reactions (IRR), bleeding events, and immunogenicity were AEs of special interest. Infections were reported in 20 (44%) and 3 (25%) pts in the 5.0 and 7.5 mg/kg arms, respectively; none were considered drug-related. Signs and symptoms indicative of IRRs were reported in 15 (33%) and 2 (17%) pts in the 5.0 and 7.5 mg/kg arms, respectively; none were grade 3/4 severity or led to treatment withdrawal. Bleeding events were rare, and none were deemed serious. No pts developed immunogenicity.
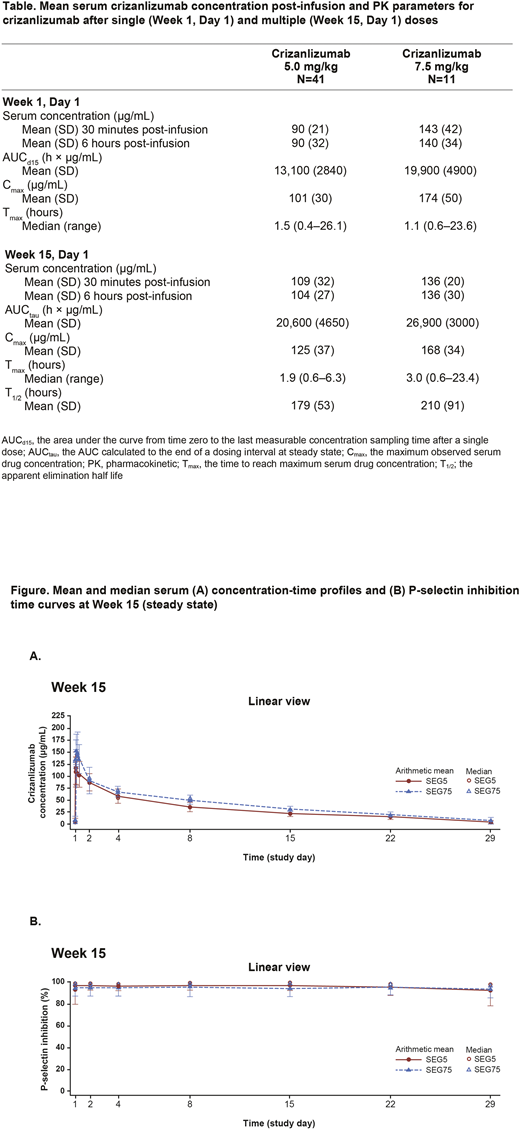
For both doses, serum crizanlizumab concentrations increased to nearly maximum levels (Cmax) at the end of the 30-minute infusion, remaining steady for 6 hours post-infusion (Figure). For each dose, Cmax at wks 1 and 15 were similar (Table), indicating a lack of accumulation. The increase in exposure to crizanlizumab in the 5.0 and 7.5 mg/kg arms was almost dose-proportional. Ex vivo inhibition of P-selectin binding to its receptor was complete throughout the dosing interval for both crizanlizumab doses (Figure). Pre-dose PK and PD were consistent and stable throughout the study.
The median (range) annualized rate of VOCs leading to a healthcare visit in the 5.0 mg/kg arm was 4.0 (1.0-25.0) at baseline and 2.8 (0.0-21.7) on treatment (median [range] absolute change from baseline, -0.97 [-14.4 to 17.7]). In the 7.5 mg/kg arm, the corresponding rates were 2.0 (1.0-9.0) and 1.8 (0.0-7.0) [median (range) absolute change from baseline, -0.80 (-3.7 to 1.0)]. Seven pts (16%) in the 5.0 mg/kg arm and 4 pts (33%) in the 7.5 mg/kg arm were VOC-free during the treatment period.
Conclusions: No new safety signals were identified in this SCD population treated with crizanlizumab, with no apparent differences between the 5.0 and 7.5 mg/kg doses in the frequency and severity of AEs. For both doses, serum crizanlizumab concentrations rose to a near maximum level shortly after infusion. Consistent with results from the SUSTAIN trial, crizanlizumab reduced from baseline the annualized rate of VOCs leading to a healthcare visit.
Smith-Whitley:Global Blood Therapeutics: Membership on an entity's Board of Directors or advisory committees; Novartis: Membership on an entity's Board of Directors or advisory committees; Prime: Other: Education material; Celgene: Membership on an entity's Board of Directors or advisory committees. Brown:Global Blood Therapeutics: Membership on an entity's Board of Directors or advisory committees, Research Funding; Imara, Inc: Consultancy, Research Funding; Novartis: Consultancy, Research Funding; Forma Therapeutics: Research Funding. Shah:Alexion: Speakers Bureau; Novartis: Consultancy, Research Funding, Speakers Bureau; Global Blood Therapeutics: Consultancy, Research Funding, Speakers Bureau; CSL Behring: Consultancy; Bluebird Bio: Consultancy. Tanaka:Novartis Institute for Biomedical Research: Current Employment, Current equity holder in publicly-traded company. Sanchez-Olle:NOVARTIS PHARMA AG: Current Employment. Albers:Novartis Pharma AG: Current Employment, Current equity holder in publicly-traded company. Kanter:Guidepoint Global: Honoraria; GLG: Honoraria; Jeffries: Honoraria; Cowen: Honoraria; Wells Fargo: Honoraria; NHLBI Sickle Cell Advisory Board: Membership on an entity's Board of Directors or advisory committees; SCDAA Medical and Research Advisory Board: Membership on an entity's Board of Directors or advisory committees; AGIOS: Membership on an entity's Board of Directors or advisory committees; BEAM: Membership on an entity's Board of Directors or advisory committees; Novartis: Consultancy; bluebird bio, inc: Consultancy, Honoraria; Sanofi: Consultancy; Medscape: Honoraria.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal